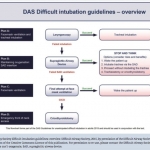
I happened to be at the World Airway Management Meeting (WAMM) in November for the 'live' release of the guidelines. We have a great deal of respect for the authors of these guidelines and the thoughtfull expertise and evidence that went into putting them together. The highlights include: 1. A focus on the unanticipated difficult intubation as opposed to an approach to the difficult airway. 2. Human factors are presented as an important contributor to difficulty and need to be addressed recognizing that airway management is a team effort. 3. For RSI, rocuronium is recognized as an equivalent if not preferred agent with acceptable speed of onset at 1.2 mg/kg and reduced O2 consumption compared to sux's energy consuming fasciculations. 4. Sugammadex is introduced as an option for the non-emergency/critical care cases with caution as it does not guarantee a return pf airway patency or adequate spontaneous ventilation. 5. Cricoid pressure still recommended during mask vent. 6. Plan A: Mask ventilation with laryngoscopy limited to 3 attempts optimized by head up positioning, with preOx and apOx, use of NMB, ELM by laryngoscopist, let up cricoid if difficult, bougie for grade 2 & 3As. 7. The choice of Laryngoscopy should be based on clinician experience but all clinicians should have access to and be experienced in alternative methods, most specifically video laryngoscopy. 8. Plan B: With declared failed plan A place a 2nd gen SGA (igel, sLMA, pLMA best evidence for) with total of 3 attempts (2 with primary chosen, 3rd with alternative). 9. If successful stop and think: awaken, continue with SGA, intubate via Flex Scope, surgical 10. Plan C: with declared failed SGA move to face-mask ventilation (FMV) and if successful awaken patient. If fail ensure adequate NMB and give FMV one more try. If unsuccessful declare CICO and go to... 11. Plan D: declare CICO ensure adequate NMB and move to front of the neck to perform scalpel bougie cric. 12. Stabilize larynx with digit 1&3 palpate CTM with digit 2 then scalpel in horizontal-rotate to vertical-bougie-tube. Use vertical landmark incision to start if CTM not easily identified. 13. Needle cric approach discouraged. All clinicians need be comfortable with a scalpel which requires regular training. All great stuff but there a few potential problems with interpretation and integration into practice as they are missing context triggers to act. More on this in my walkabout talkabout.
 I happened to be at the World Airway Management Meeting (WAMM) in November for the 'live' release of the guidelines. We have a great deal of respect for the authors of these guidelines and the thoughtfull expertise and evidence that went into putting them together. The highlights include:
I happened to be at the World Airway Management Meeting (WAMM) in November for the 'live' release of the guidelines. We have a great deal of respect for the authors of these guidelines and the thoughtfull expertise and evidence that went into putting them together. The highlights include: