Awake Intubation after Topicalization of the/my airway and the Penetrating Neck Injury
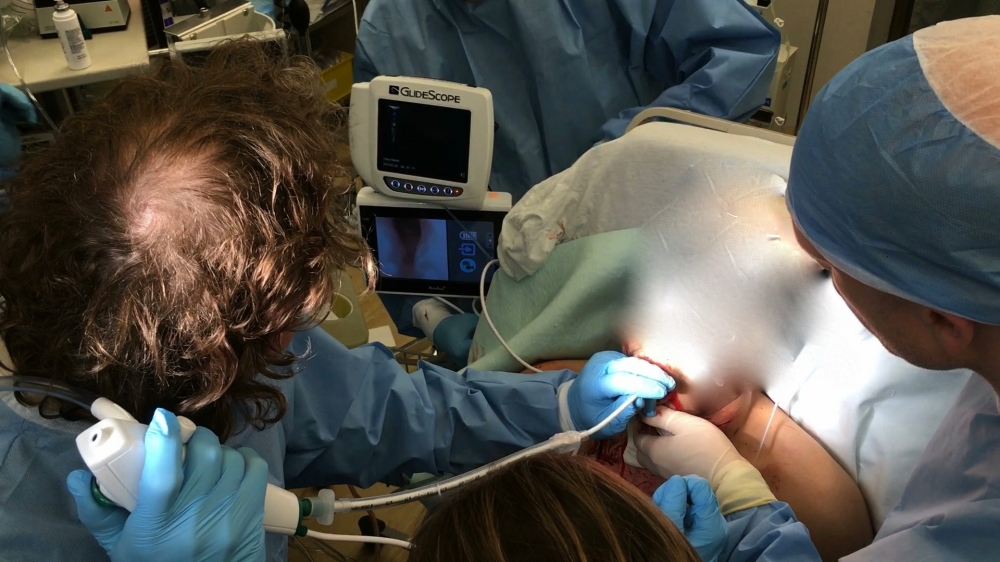
Several years ago we reviewed a paper presenting a case series of airway management in the penetrating neck injured patient. The conclusion was that RSI was safe and the preferred technique for managing PNI. Maybe, but this series and others like it have not answered the real question... what is the safest approach for managing a primary or secondarily (hematoma) injured/distorted airway. You can do what ever you want with a hole in the neck but what about a hole in the airway? Most of these patients had a hole in the neck but the incidence of actual airway injury or distortion was unknown. Prospectively knowing whether the airway is involved is either obvious or not. Why do we have this need to paralyze everybody... yes its easier and has a higher success rate but the easy approach isn't always the best. Ideally for the PNI patient the technique should involve a visual of the airway beyond the point of injury. Blind passage of an ETT or bougie can potentially turn a partial airway injury into a complete one. Positive pressure ventilation before the airway is secured can cause significant subcutaneous emphysema and further distort the airway. My approach is to do these patients awake. If this is not possible a 'triple set up' with the neck prepped, a King Vision/Flex Intubating Scope combo is my go to if I have to do an RSI. Here is the case... I used the recipe described in the previous post and intubated the patient using awake topicalization and an Ambu aScope. The key was proper topicalization as demonstrated in this selfie intubation.