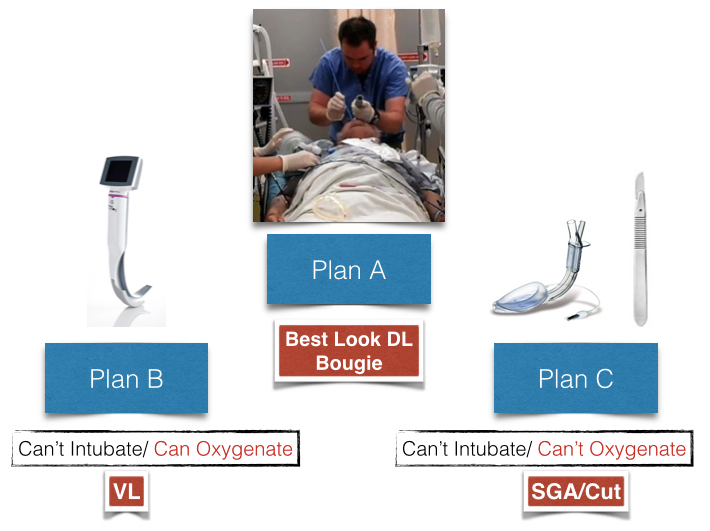
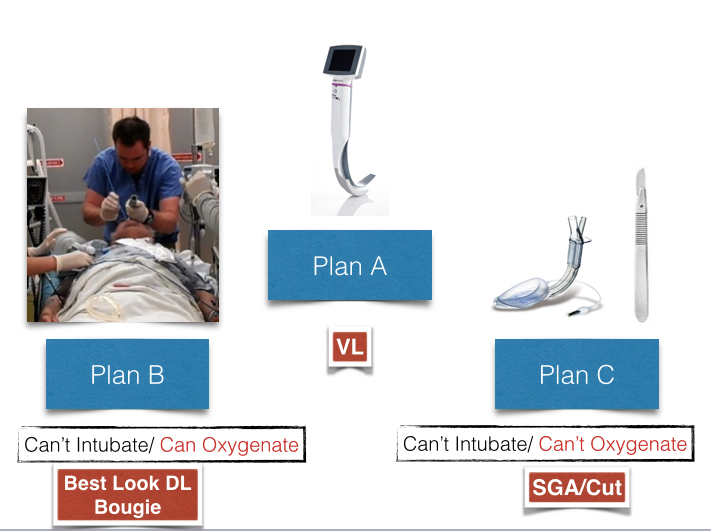
We get asked quite frequently to wade in on the DL versus VL debate, the new versus old, the obsolete versus the irrelevant and even the standard of care versus the dangerous. There are very strong views on this subject to the point that some feel we are wasting their time by teaching the dying art of direct laryngoscopy. I could present my opinion, supported by the evidence or state that we should wait for a Cochrane review but none of this really matters. As I stated in an editorial "VL... is not a 'magic bullet; it is a device option, and when used by the right person, in the right situation, on the right patient, it may be of value." As Rich Levitan has said we haven't done away with seatbelts because of the airbag. This gets to my simple answer in addressing this controversy. Its about having a Plan A, B and C that works for you and the patient. Lets get plan C off the table- it is your rescue oxygenation strategy for can't intubate/oxygenate which demands a commitment to an ESA with an option for SGA (2nd gen) placement if appropriate. Plan A is your initial approach, which for some is Best Look DL/Bougie and for others is VL. If Plan A fails then it is plan B (can't intubate/can oxygenate with BVM) which again is usually Best Look DL/Bougie if VL failed with plan A or VL if Best Look DL/Bougie failed with Plan A. Everyone is looking for the airway AED equivalent but It doesn't exist. We have to be just as good for our plan A as we are for our plan B (DL rescues VL, VL rescues DL). The very concerning data that seems to be buried in the literature comparing DL and VL is the falling 1st attempt success rates for DL. Our technologic preference is likely contributing this observed DL skill decay. There is no button we would push to choose a seatbelt over an airbag, ensuring optimal patient outcomes requires both!